Content
- Abstract
- Keywords
- Background
- Regulation of the immune responses and implications in the antineoplastic defence
- The cooperation between APC/Th
- Signalling possibilities in malignant clones and in parallel in leukocyte clones involved in the antineoplastic defence
- Activating signals in the immune system
- Signaling cascades in neoplasms
- The impact on neoplastic tissues
- The impact of physical radiation on tissues
- Impact on the immune system
- Parallelism between the immunological tolerance induced by pregnancy and tolerance in neoplasm
- References
During the intervention of the immune system in the antineoplastic defence, it is not known exactly how to capture, process and present neoplastic antigens at the level of APC (antigen presenting cell) and they may not be correctly presented to the Th lymphocyte, because it would trigger a strong response to reject the malignant cell from the onset of neoplasia.
Therefore, the major immunological defect in neoplasms may be rather in the specific immune system, related to the cooperation APC/Th, while the Tc lymphocyte may be less affected, but it may not function correctly in the absence of the stimulation Th1 lymphocyte by IL-2 . In this case the lymphocytes Tc are deleted (the deletion is mediated mainly by ).
Also, receptors for neoplastic antigens are not described in APC, and some of these antigens are probably taken by opsonization with antibodies or complement fractions, while others are taken as detritus (from dead neoplastic cells) in scavenger receptors ( involved in clearance, apoptosis, homeostasis).
The immune response of the Th lymphocytes and especially Th1 is, however, poorly related to the extremely aberrant degree in the neoplastic cells and it may be more focused on the antigens from dead tumor cells. On the other hand, on the living neoplastic cells, the Th lymphocytes cannot recognize them well and annihilate, probably through a pathological tolerance process.
Keywords: helper T lymphocyte (Th) , reglulatory T cells (T regs) , cytotoxic T lymphocyte (Tc ) , APC – antigen presenting cell, APC / Th cooperation, MHC-I cup, MHC-II cup, NK lymphocytes , T cell receptor (TCR), interleukin 2 (IL-2), stimulatory signals, co-stimulatory molecules, adhesion molecules, “signaling cascades”.
A proof of this is the attempts to use vaccines with dead tumor cells, as well as the good response of chemotherapy and radiotherapy, where massive tumor necrosis occurs. It is possible that high efficiency also results from a participation of the immune system, especially since cytostatic secondary immunosuppression is practically not as high as it was theoretically described, especially in the case of Cyclophosphamide , that can be used in oncology in very high doses with good tolerance (versus the immunosuppressive doses in the autoimmune pathology). Also in some forms of nodular breast cancer, it is preferred to do the conservative intervention of sectorial type, by keeping the surrounding tissue, possibly with a role in the stimulation of the immune system by the remaining tissue.
As for the nonspecific immunity, it seems less affected and the NK lymphocytes are mostly involved, they ascend and take the first place in the antitumor defence probably because they act without MHC restriction. Therefore, if Th1 is significantly affected, the lymphocytes Tc, which would be the basis of the antitumor defence, can no longer function normally; instead the NK lymphocytes can do it, they enter the specific defence. In addition, the B lymphocytes can do it and they are dependent on Th2 and have normal lines to work T independently. Among the NK lymphocytes and some Tc , were selected the LAK (Lymphokine Activated Lymphocytes), whose cytotoxic activity is increased by the increased expression of adhesion molecules following IL-2 activation.
In time, it seems that the B lymphocytes have become more specialized in the production of monoclonal antibodies increasingly effective, with therapeutic implications. Many of these B lymphocytes may be coordinated by Th2 or T independent (given the defect in Th1 ) ; these, similarly to the NK lymphocytes, have risen so that tumoral immunity has been among the first places in the antineoplastic defense.
It seems that the non-specific immunity is less affected and works better, but it does not have such a large capacity because it has no specificity. The macrophages / monocytes are involved, the eosinophils that have important antitumor cytotoxic activity, the neutrophils that destroy especially the metastatic cells in the circulation, while the complement system is less described.
The macrophages have still unknown mechanisms to destroy the tumor cell and to process them as APC , which may be one of the main unexplained links in the cellular mechanisms. It seems that the cytolysis of the neoplastic cells is not obtained by phagocytosis, but by cytotoxic substances: TNF-α produced by macrophages, lysosomal enzymes such as serine proteases, oxygen peroxide, IL-1. They act especially by inducing apoptosis (programmed death), unlike the NK and Tc lymphocytes that induce lysis death (by cell-cell contact and by the membrane perforation mechanisms). The main lymphotoxin of the NK and Tc lymphocytes is TNF-β.
In the case of NK lymphocytes, the genetic determinism matters (their number and activity are genetically conditioned). However, paradoxically, as the disease progresses, their number decreases in the final stages probably by the intervention of the hyperactivated suppressive T lymphocytes .This means that some suppressive mechanisms related to the Treg lymphocytes are probably the coordination (help) from Th, so from the highest level and which are most likely related to the impossibility of the APC / couple to initiate a correct response.
The immune system, at least at the onset of most neoplasms, seems intact, so the alleged defect may be only functional, which means that the main superior lymphocytes, Th1 and Treg , do not “see” the neoplastic cells or they have established from the beginning total tolerance to these cells, which resembles the tolerance in pregnancy. The pathological tolerance process, which seems an accidental phenomenon, may have started from the highest level, from Th1 and Treg , then it was decreased or blocked, so that the Tc lymphocyte can still function (but it does not have the maximum capacity because it does not have good stimulation from by IL-2). Subsequently, the Th2 lymphocytes and the B lymphocytes, including the independent T lymphocytes, seem to function better, whereas the NK lymphocytes, which are not so dependent on Th1 (they have only help by IFN-γ), ascend to the first line whereas macrophages / monocytes, eosinophils and neutrophils participate well in the non-specific defense.
The activated macrophages are known to have high cytotoxic power against a multitude of cancer cells. The main secreted cytokine is TNF-α, whereas IFN-γ, the main effector cytokine of the Th1 lymphocyte, has been found in several studies to be less efficient, so it seems a kind of inversion, which means that they ascended the lower elements of the non-specific immune system, having in view that the upper main lines have a major defect.
Some specialists have previously suggested that neoplastic cells are coated with antibodies, which would make it impossible to recognize them, but it seems that there is a different charge (electrical, magnetic or electromagnetic) on these cells that is present in the in situ stage from the first appeared neoplastic cell. If this charge (radiation) is somehow similar to the charge of the egg cell, it could confuse the Th lymphocyte and trigger a signal to induce tolerance as in pregnancy, by an unknown mechanism, the induction of the pregnancy tolerance, which is certainly triggered by the egg cell and it spreads to all the embryo-fetal cells. If the first neoplastic cell accidentally carries a signal (electrical, magnetic or electromagnetic) that resembles or imitates the signal of the egg cell, it could explain the lack of the tumor rejection.
The NK cells, especially at the placental level, also play a central role in the pathology to reject pregnancy .
Regulation of the immune responses and implications in the antineoplastic defence
Regulation at the level of Th1 lymphocyte is preponderantly autocrine made by IL-2 that acts upon the IL-2 receptors : IL-2R, CD 25 ( scheme no. 1) .
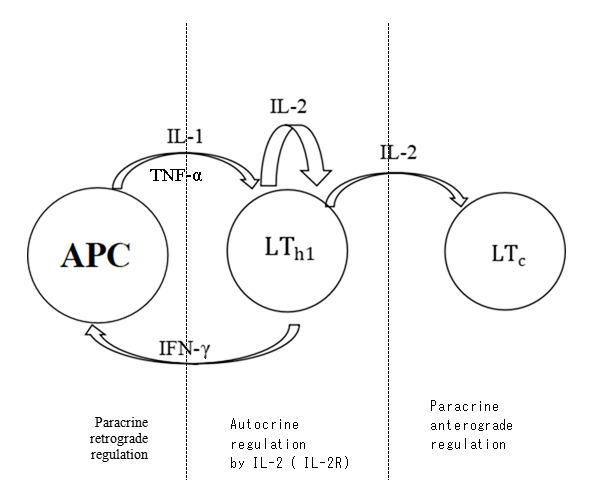
Scheme no. 1: Regulation of specific cellular immune responses at the level of the Th1 lymphocyte
APC – antigen presenting cell
L – lymphocyte
L – cytotoxic T lymphocyte
IL-1 interleukin 1
IL-2 interleukin 2
IL-2R receptors IL-2
TNF-α tumour necrosis factor
IFN- γ interferon γ
IL-2 is used by in the main anterograde coordination (help) functions at the level of Tc and at the level of NK lymphocytes and macrophages together with IFN-ɣ. The receptor for IL-2 is CD-25, the main marker of the Treg lymphocyte , so it is a kind of argument that IL-2 can successfully participate in mechanisms of regulation and self-regulation and it is known that it activates most of the cellular immune responses in which is involved.
The Tregs CD4 + CD25hi+ Foxp3+ that have mainly a suppressive role, use IL-2 as the main regulatory interleukine, where as the lymphocytes Th1 use IL-2 for the auto-regulation. Therefore, the Th1 lymphocytes , by the help function, may also intervene in the coordination of the Tregs. There are two types of Tregs lymphocytes: native and acquired.
The CD4+ Tregs lymphocytes having a common way of differetiation with CD4+ T helper lymphocytes ( with Th17 ) who are help , effector and with memory , that is possible as sometime it not may exercise well the supressor fonction .Tregs express similar phenotype with the effector cells activated CD4+CD25+ ( which have effector functions ) .
Classic , at the beginning of the immunolgy , it was discribed that having supressor fonction the T supressor lymphocyte Ts CD8+ , then some authors have atributed the supressor rol of the Th1 lymphocyte , which inhibit Th2 ( by IFN-γ) and of the Th2 lymphocyte which inhibit Th1 by IL-10 ( which is also principal supressor cytokine utilized by regulatory T lymphocyte ); in present the principal rol of supressor is atributed of the Tregs cells .
Tregs cells inhibit : autoreactive CD4+ T cells (role in autoimmune diseases ) , immune responses antitumoral , effectorT cells ( in the chronic infectiosis diseases ) and alloreactive Tcells (in transplant ) . The Tregs cells inhibit also the lymphocytes Th2 , but our function in allergic inhibation pathology was not established always with certainty .
Some studies have demonstrated the presence in the cancers of T supressor linies CD8+Foxp3+ ( in the cancer of prostate ) .
Is interesting why supressor T lymphocytes were described initial by well known immunologists as belonging to CD8+ subset ? It possible as the numbers of these be decreased in time? It possible be increased in parallel the number of the supressor lymphocytes CD4+CD25+ which are also involved in the immunological tolerance , possible also because of in late period the increase the number of immunogenes and allergenes ( because of the industrialization ) . It is possible as in the epoch of industrialization work supressor CD4+ cells , while formarly has worked supressor CD8+ cells (more stable ) ?
In neoplasia , the Tregs cells are increasedand inhibit the antitumoral activity , which should be favorable . Tregs in cancer don’t differ as phenotype of other Tregs cells .
New strategies of traitement visa on the manipulation of the Tregs cells in the immunotherapy against cancer ; also , the activation cytotoxic Tcells have good efficacy ( of the type CAR-T cell therapy) , or possible manipulation of the some therapies at level of Th lymphocytes , eventually with the perfection of the APC/Th cooperation ,
The cooperation between APC/Th
Returning at the cooperation between APC and Th1 , which is one of the important links of immune response , is interesting, that, in the retrograde coordination at the APC level, the participation of IL-2 is not described in the literature, but only the participation of IFN-ɣ (the increase in the expression of MHC-II) is described. This is a cytokine with the main effect function and it would have been expected that IL-2 participated, too, especially since it is the main interleukin regulating macrophage along with IFN-ɣ. The macrophage is part of the nonspecific defense and its role is smaller, while the APC participates in a superior function of taking, processing and presenting antigens to helper lymphocytes, which is a key function to initiate and develop immune responses, but it is not known why its coordination at the higher level of is made only through IFN-ɣ.
Conversely, APC and macrophage go with the same stimulation on , mainly with IL-1, and they have almost the same cytokine profile: IL-1, IL-6, IL-8, TNF-α, IL-12, IL-23 for APC and IL-1, TNF-α and IL-6 for macrophage.
One of the main functions of the lymphocyte as “the general” of the immune system is the function of stimulation (help) at the level of , made mainly by IL-2. The other roles of regulating the macrophage, the NK cells or the lymphocytes seem minor, whereas the Th / interaction seems to be one of the main links which would illustrate the fact that both of them could be considered “generals” of the immune system.
This would be the basis of the antitumor defence because lymphocytes are deleted in the absence of Th (deletion is mediated by ).
This seems to be precisely the case with neoplasms, as it is not well known how to process tumor antigens at the APC level and whether the presentation to Th is efficient. In this context, NK lymphocytes are part of the nonspecific defense and can probably still function if Th (and implicitly Tc, too) have problems, they specialize better and some become LAK lymphocytes, which reach the first line, possibly more efficient than (classically, NK lymphocytes were described as the third line, after T and B lymphocytes). At the beginning of immunology, they were considered to be part of the non-specific defence or borderline defence, then in recent years they have risen and in some cases they function specifically.
Also, in the antineoplastic defence, all the elements of the non-specific immune system have risen, including the eosinophil, probably through the blockage that seems to exist in the upper Th lymphocytes. It is interesting that the eosinophil is also the cell that responds and proliferates in case of exposure to high X radiation levels, and there are cases of hypereosinophils in radiologists who had prolonged exposures to radioscopes.
The elements of the non-specific immune system, especially neutrophils, also deal with metastatic blood cells.
From some studies it results that IFN-ɣ produced by the lymphocyte is not very efficient in the defence against tumors.
On the other hand, in most neoplasias, the immune system does not seem to have immunodeppression at the beginning of the neoplasia, but it installs it along the way.
This would mean that there could be a “functional” blockage even in the “general” Th lymphocytes (respectively at recognition at the presentation of APC), which would explain the uncontrolled evolution of the disease with massive metastatic invasion.
Also, Th1 lymphocytes may have a blockage and Th2 and independent B cell activation increase and they seem to have specialized in time and offer more and more efficient models of monoclonal antibodies with therapeutic implications.
Recently, it seems that the efficiency of antineoplastic defenses on all lines of the immune system increased because the overall evolution of malignant conditions is better.
Signalling possibilities in malignant clones and in parallel in leukocyte clones involved in the antineoplastic defence
The Th lymphocyte has a kind of immunological “isolation”, namely it never comes in direct contact with anyone, neither with antigens (only through APC) nor with other cells (only through interleukins), whereas the regulation does it rather autocrine by itself (more often through IL-2). All of them are probably part of a complex protection mechanism so that it cannot be disrupted.
The main characteristic of the lymphocyte is to function by the recognition of antigens in the MHC I cup of the target cells; however, it needs a confirmation from the lymphocyte, which is recognized in the MHC II cup of APC and acts as a help on Tc, so practically lymphocytes need the double recognition, because in the absence of they are deleted.
It is interesting that this / cooperation, which seems to be of major importance in the development of immune responses, is less known and less described in immunology and it is achieved mainly through IL-2.
Also, the help function exerted by the Th1 lymphocyte on APC, which is also of major importance, is less known and mainly performed on IFN-γ.
It is possible that, in addition to the classical molecular systems described (interleukins and intercellular interrelationships at the level of the receptor), there appears an additional system of intercellular signaling, possibly physical, even physical radiation that doubles the chemical one, given the rapidity with which the signaling sometimes spreads to all the elements of the immune system.
The immune system may have an intelligence that enables it to make more complex analyzes than the ones known classically, namely that it may also analyze various radiations or more complex physical and chemical signals through a signaling system that is more complex than the classically described one.
A theoretical example would be the rapid spread of the signal from the first Th lymphocytes that come into touch with the antigen (in the MHC II cup of APC); the activation and transformation signal into effector and memory lymphocyte or, if necessary, the deletion signal spreads rapidly to the entire Th lymphocyte clone no matter where it is located in the body, so there may be a physical signaling system in addition to the classical one, which is more of a chemical type, through molecules and cytokines (messenger molecules of the immune system).
Classically, the signaling between the elements of the immune system is made:
1) through close contact between cells – intercellular interrelationships established at the level of surface receptors, which involves the main signal plus several secondary, co-stimulatory signals and
2) by interleukins that have an autocrine action (on the producing cell), paracrine (on the adjacent cells), and some authors describe the endocrine function, at a distance from the secretion place.
The signaling and the communication of the elements of the immune system at a distance is less known but it seems to be of major importance.
Similarly in the case of CD8 + lymphocyte, if a certain number of Tc lymphocytes are locally engaged in an offensive reaction by the recognition of antigenic determinants in the MHC I cup, there is probably a rapid signaling at a distance by which all the Tc clones are informed about the immune status. These signals can be physical in addition to the chemical ones.
It is possible that such signals also work in the malignant clones, because all the malignant cells seem to bear the same signals that were originally on the first malignant transformed cell.
Also in pregnancy, which is a semiallograft or even an allograft in the case of carrier mothers, the immunological tolerance is established for a period of nine months immediately after the formation of the egg cell, and it is extended to all the elements of the immune system. It is not known by what mechanism, but the pregnancy tolerance is established quickly because the egg cell and all cells derived from it must not be attacked by the elements of the immune system, especially the local ones, most of which are part of the nonspecific defence.
Probably here, in addition to the classical system described by the molecules (cytokines, hormones, enzymes, proteins), there is also a physical signaling system, especially between the cells of the immune system, given the speed with which the pregnancy tolerance must be established.
Activating signals in the immune system
As for the immune system, the main types of signals involved in inducing and keeping immune responses are:
– the main signals from the interaction between peptide-MHC and TCR / , which are activators and are transmitted to the depth of the cytoplasm
– the signals at the level of the co-receptors (, , that have the role of stimulating adhesion and transducing signals); the co-stimulating secondary signals must be present simultaneously with the main ones
– the signals transduced by the accessory molecules; these molecules are the same for all the T lymphocytes and have no ability to recognize the antigens; they simply have a role in adhesion.
Classically the T and B lymphocytes require two extracellular signals in order to be activated. For the T lymphocytes, the first signal is conferred by the interaction between the peptide -MHC complex with TCR (and the co-receptors or ). The second signal is given by the co-stimulatory molecules expressed by APC and that have interactions with specific receptors belonging to the T cell.
The way TCR/CD3 is the main way to signal (main signals), while the co-stimulatory (secondary) signals are transmitted to other co-stimulatory molecules, which are expressed by APC and interact with the specific receptors of the T lymphocites (for example – ). The co-stimulatory signals must be present simultaneously with the signals induced by the antigen.
The absence of co-stimulation, having in view the presence of the antigen, can determine the elimination of the T lymphocyte by inducing the death of the cell or by inducing anergiy (non-responsivity).
The T lymphocytes also express some accessory molecules that are identical to all T cells and do not have the ability to recognize the antigen, but they interact with various molecules (ligands) in APC (for example CD2-LFA3 and LFA1-ICAM), target cells or vascular endothelium, and also play a role in homing.
The adhesion molecules also play an important role in the LAK lymphocytes, whereas their expression is increased by IL-2, with a role in binding the target cell and triggering the cytotoxic effect.
The accessory molecules are also used as surface markers in the immunohistochemical identification of the T cells in different conditions (leukemia or lymphomas) .
These adhesion molecules may play a role in transmitting the signals at a distance, because they have a time-related criterion (the role of establishing a long enough contact between cells, which enables the making of the functional interactions) and a space-related criterion (they are identical in all the T lymphocytes, they have no polymorphism).
The transduction of the signal at the level of the co-receptor molecule involves a classical example of chemical molecular signaling at the level of the immune system: the intervention of protein tyrosine kinase belonging to the family src called Lck, that are specific to the T lymphocytes and are associated to the cytoplasmic tails belonging to the co-receptor molecules. Lck acts to phosphorylate the chains of complex to tyrosine residues when the cytoplasmic tails of or interact with the ones of the TCR-complex in the recognition process of the antigen.
This tyrosine phosphorylation in the cytoplasmic tails of occurs in the enzymatic cascade that is necessary for the activation of the T lymphocytes.
The main enzymatic cascade during the activation of the T lymphocytes is the cascade of the phosphatidylinositols and the principale protein tyrosine kinase is PTK p56 lck.
The cooperation between the Th and APC lymphocytes has as a basic element the polarization of the Th lymphocytes versus APC at the level of the membrane and of the level of the cytoplasma, a phenomenon called by the immunologists “the immunological synapsis’’ (the supramolecular activation centre SMAC ) .
This polarization is of a physical type but also of a chemical type, therefore the immunological synapsis can represent a model of double signaling in intercellular relations.
As for the connections present in the antigen-antibody complex, which is the basic element to trigger the immune response, they are not covalent, therefore relatively weak and reversible:
– electrostatic (ionic) bonds emerge between ionic groups with opposite electric charges (as in the case of , )
– hydrogen bonds emerge between atoms that are negatively charged and belong to polar molecules () and hydrogen ions that have a positive charge () and belong to hydrophilic groups (OH, ). These hydrogen bridges are based on electrostatic interactions and are weak.
– the bonds of van der Waals are represented by attraction forces emerged as a result of the interaction between the external electronic clouds at the level of the respective molecules
– hydrophobic bonds emerge between nonpolar molecules as they approach each other during this process and eliminate water molecules between them.
Signaling cascades in neoplasms
It is interesting that in oncology the most frequently described signaling ways are represented by the binding of the ligand (most often the growth factor) to the specific receptor (the extracellular domain), which results in the mobilization of proteins and enzymes with a role in activating the intracellular cascade, whereas some tyrosine protein kinase src are also described as proto-oncogenic.
Clasically there are “signaling cascades“ with a regulatory role in the tumor growth, proliferation or apoptosis, whereas deciphering the mechanisms of these cascades, of the transduction of the signals and of the proteic interactions is used in the initiation of the biological therapies that act on the molecular mechanisms (signaling ways, growth regulation, cellular cycle, expression of genes, angiogenesis, apoptosis) .
The main signaling ways in neoplastic are the way of the epidermal growth factor receptor (EGFR) and the way of the vascular endothelial growth receptor (VEGFR) .
The main targeted therapies are monoclonal antibodies (mabs), directed mainly against the receptors of the growth factor (extracellular domains) or inhibitors of to the thyrozinkinase domain, used in the inhibition of the intracellular signaling way (small molecules) or the blockers of the transduction signal (like the inhibitors of ras way) or modulators of the cellular cycle, inhibitors of angiogenesis or inductors of apoptosis.
Most of the signaling types described in neoplasms are chemical, but it is crucial the disruption of the cellular cycle, of the growth ways and proliferative signalling that include growth ligands, its receptors or signalling molecules. One of the most important is the transforming growth factor TGF-β, which is also an important citokine in the regulation of the immune responses..
Also, during the metastasis and invasion of cancer cells, there were descriptions of several molecules that have complex roles and may have signalling functions: proteoglycans, fibronectin, collagen, elastin, laminins, various proteinases and glycoproteins. Some enzymes such as matrix metalloproteinases (MMP) are important in the invasion, they are high in many cancers and have a poor prognosis significance.
The chemicals known to be involved in tumorogenesis are multivarious from the exogenous ones, including nutrients or molecules of microbial origin (oncogenic viruses, bacteria such as Helicobacter Pylori) to endogenous ones, including metabolites (“oncometabolites”).
Theoretically, one may initially describe a signal or a multitude of neoplasia-inducing signals that trouble the first neoplastic cell; this signal are unknown (according to some authors, it is necessary the affecting some cells belonging to the same tissue in order to trigger a neoplasm), followed by one or several signs of the progressing tumor.
Following the inductive neoplasm signal, which is unknown, a complex signaling cascade seems to be triggered (’’signaling nets“) that are better known and described classically within the signaling pathways at the extracellular level and at the intracellular level.
Regarding the inductive signal, it could be a chemical one or a physical one or both together, possibly acting by summation, which would represent a variant of the theory of the two signals. It is about chemical or physical induction signals, not neoplasms induced by chemical substances, which are classically described as having a latency period of approximately 10 years since the exposure or the ones induced by radiations that require approximately 20 years since the exposure to triggering.
The first cell affected neoplastically by this signal may by exclude itself by deletion as a protective mechanism. It could work for the following 2, 3, 4 or 5 cells (the signal ’’jumps“ from the dead cell to another one until one fails, can no longer delete itself and becomes the promoter of the malignant clone, an aspect suggested in the theory of the clonal deletion).
Also, the signal may be present on the neoplastic cell (respectively on the whole malignant clone derived from it, including the metastatic cells) and on the immune system, on all the leukocyte clones involved in the antineoplastic defence, which would represent another variant of the duality of the theory of the two signals (the signal present in parallel on the neoplastic clone and on the leukocyte clones dealing with them, both showing disorders. Only the malignant clone has important organic and functional disorders, whereas the leukocyte clone has only functional disorders) .
The impact on neoplastic tissues
This sign inducing neoplasia may be physical, chemical, or both together, but the etiology is currently unknown.
Arguments for the involvement of physical signals (radiation) in the etiopathogenesis of cancer:
1)the carcinogenic effect of high frequency radiation such as γ or X, infrared or ultraviolet is known, whereas the involvement of medium frequency radiation such as electromagnetic waves is debatable; the involvement of electric or magnetic fields is also debatable as several authors discuss magnetic disorders in the neoplastic cell.
2) it is interesting that the adipose tissue does not develop in malignant tumors and it is known that in ultrasonography it reflects ultrasound more strongly; thus it can be deduced that, if it reflected the radiation involved in inducing the neoplasm, it would increase the malignancy risk in general and in the surrounding tissues (for example: breast cancer ranks first place in women when breasts in many women have an important fat component; also in men one the first places is occupied by prostate cancer that may be related to the lipid load of the prostate. However, it is considered that the capsule has no malignant transformations in the structure of the prostate.
One of the first places is occupied by the neoplasm of the colon and it is also linked to the excessive fat consumption, whereas obesity increases the general risk of neoplasms.
Mesenteric ganglions are very much affected in neoplasms, possibly due to their proximity to the retroperitoneal fat.
It should be noted that two of the main symptoms of neoplasms are weight loss, which can lead to cachexia and the loss of appetite; they may be one of the mechanisms activated especially for the defence (getting rid of the adipose tissue). These symptoms were common in the past, but have recently worsened and are less common.
Interestingly, there are two tissues that seem to cause neoplasms: the adipose tissue and the embryo-fetal tissue in the embryo and fetus; the latter has ultrasonography as the imaging disgnostic method, as well as neoplastic tissue. The described embryonic tumors are at the level of the placental elements, and if the pregnant mother has a neoplasm, it seems that the risk of spreading to the embryo or to the fetus is low.
The embryonic tumors usually develop in adults from embryonic remains, whereas in the embryo and fetus neoplastic tumors seem to be more developed from the maternal elements.
The impact of physical radiation on tissues
As for high frequency physical radiation, it is known to be carcinogenic, however those with radiodiagnosis or radiotherapeutic implications at standard doses do not seem to be inducers of neoplasms (arguably in the case of radiotherapy which may be considered as chemotherapy, inducers of second neoplasia, especially lymphoma, after several years).
In contrast, X-rays widely used in radiodiagnosis, including pediatrics, do not seem to be inducers of neoplasms.
Even in the case of CT (computed tomography), where the dose can be bigger to 40 times in comparison to the standard radiography, the risk of neoplasia is not considered.
One of the explanations could be that in the case of CT the dose is received all at once, so it is not equivalent to 40 times the exposure .
This might mean that it is only a component of the radiations that is received at the moment of the emission, so that if it is emitted once (CT), it is received, and if it were emitted for 40 radiographs this component would be received 40 times, which would not even be possible to do in practice .
If there is only one carcinogenic component in these radiations, it might explain the differences between the radiations used for medical purposes and other types of radiations.
Also, this might explain the high doses of γ radiation used in radiotherapy, which, however, do not usually induce malignancy, but what occurs after several years cannot be known exactly if it is the second neoplasm or it is just a recurrence. It is interesting that radiotherapy can be concomitantly associated with chemotherapy without aggravating such as severe immunodepression.
In the past the specialists recommended not to repeat the radiographs in 6 months after a classical exposure but currently there is no longer such a restriction, probably it is a resistance to the X-rays that progressed in time. However, if there is only a carcinogenic component of X-rays, it may have remained confined to the body for approximately 6 months until its disintegration. The patient with external radiotherapy does not become radioactive and is not dangerous to those around him, however it is not known if this patient does not remain at the level of risky tissues for him, given that a neoplasm might occur after several years.
However, in present this 6 month restriction no longer applies , so that X-rays can be taken even after CT exposure . Is may be possible that the very high doses during the exposure to CT push this carcinogenic component so that it does not get attached to tissues?
Is it possible that the same thing happen to the high doses used in radiotherapy when the said component does not get attached to tissues?
As for the natural background of radiation, it does not seem to be involved in the etiology of neoplasms. However, in geographical areas where it is higher (it can be even double), it is considered a higher risk.
Going down the scale of radiations frequency, this carcinogenic component is weakes to some medium electromagnetic frequencies and it is not described at low frequency radiations.
However, there are multiple interferences with average to low frequency radiations and also to the low frequency ones. Theoretically radioablation would be one of the most efficient of the physical methods, as well as cryotherapy. They both show great differences between theory and practice because they practically do not have the expected efficiency.
However, it seems that there are interferences between radio waves and neoplasia signals, but in the case of cryotherapy it probably modifies the cellular electrical potentials and produces physical interferences in the signal. These interferences also occur in case of temperature increases:
– thermography is sometimes used to diagnose breast cancer
– the increase in the temperature by one degree in the not lowered testicle increases the risk of malignancy
– the high fever episodes, with 40 degree Celsius, destroy some tumor cells, whereas many neoplasms evolve at the same time with fever, secreting pyrethroids as a defence mechanism.
There are also interferences with the electric and magnetic fields and attempts of regulating therapeutic interventions by magnetic fields.
When analyzing the low frequency radiations, they are not described as carcinogenic, however they seem to have interferences with them. Ultrasonography is one of the choice methods in the diagnosis of neoplasms, while in the close range, the radio waves could be efficient to annihilate neoplasms.
This would mean that the neoplastic tissues may carry radiation with frequencies close to them but different from the classical known ones that belong to the technical field. Is it possible that these radiations belong only to living cells? However, the carcinogenic component is also found in high-frequency radiations, so it may be mixed, emitted by living cells, objects or cosmic and telluric radiation.
The said signal is not among those known with low frequencies, but that is why there is the possibility to be itself with low frequencies and to show incompatibilities to associate with them, expressing only some interferences. In the case of ultrasounds it would be a kind of imaging detection and possible reflection as in the case of the adipose and embryo-fetal tissue, but in the case of radio waves it would have the opposite effect of annihilation.
A good imaging expression in the case of malignant tumors is shown by the X-rays (radiography, radioscopy, CT), the magnetic resonance imaging, scintigraphy and also methods that combine physical X-rays with chemical metabolic changes induced by the administration of chemical solutions (PET-CT). Radiomics consists in the correlation of several dates extracted from medical imaging techniques (CT, MRI, PET-CT, RD digital radiography, ultrasonography) with clinical dates and biological dates in order to find a diagnosis and a therapeutic decision with maximum benefit .
It is interesting that some animals (dogs) having greater instincts and perception abilities of some types of waves ( ultrasounds ) have been used by research teams in attempts to diagnose malignancies.
All this suggests that certain radioactive physical signals may be involved in the etiopathogenesis of neoplasms and in the interference with various methods of diagnosis and treatment. Thus, in the etiopathogenesis of neoplasms, a physical inducing signal doubled by a chemical one may be involved, which at the cellular level (at the moment of the impact) goes through a conversion, so that later (as a progression signal) it is expressed more by the chemical signals that are described classically (“signaling cascades”).
The eosinophil is a cell that plays an important role in the non-specific defence in antineoplastic defence and it also seems to be a cell that has numerical increases in the presence of radiation (eosinophil increases have been present in radiologists who have had high exposure to radioscopes and angiographies ) .
Hypereosinophilia is also found in parasitosis, especially in the case of helminths that are larger than protozoa and may have a radiation charge harmful to the host organism.
The bilobate nucleus of the eosinophil could be an additional argument, because for radiologists the first signs of prolonged exposure to radiation are fragment leukocyte nuclei. The cells involved in the defence against the malignant cells in the circulatory stream are neutrophilic polymorphonuclei which may detect a radiation charge specific to the metastatic cells.
The exploration of the immune system is made by various physical methods (precipitation, agglutination, immunofluorescence reactions, solid phase tests: Radio Immuno Assay (RIA), Radioimmunosorbent test (RIST), Radioallergosorbent test (RAST), Enzyme Linked Immunosorbent Assay (ELISA) , immunohistochemistry, molecular biology techniques. All of them include chemical methods, especially enzymology, whereas flow cytometry is the choice method in the identification and analysis of the lymphocyte populations and the method of immunological choice in hematological malignancies (the immunophenotyping collects the information obtained by the recorded signals) by fluorescence emitted by fluorochromes coupled in most cases with monoclonal antibodies specific to the epitopes of the respective cell passing through the laser beam).
The multitude of physical and chemical techniques used in immunology denotes multiple interactions of this order between the elements of the immune system.
It should be noted that the immunophenotyping and the analysis of the CD system (the cluster of differentiation), especially of the populations of CD4 + helper T and CD8 + cytotoxic T lymphocyte is made at choice by using laser electromagnetic radiation in flow cytometry, therefore the interactions are electromagnetic and chemical.
Regarding the cooperation between the T lymphocyte and APC, there is a polarization of the T lymphocyte in relation to APC in the membrane and in the cytoplasm, which represents “the immunological synapse”.
Dendritic cells , besides the functions of antigen processing and presentation and cytokine production , also have roles of T-cell polarization .
One of the basic elements is the antigen-antibody bond which is non-covalent, relatively weak and therefore reversible.
If, in the case of neurons and in the case of interneuronal synapses or neuro-motor plates, there are changes in the electrical potential of the membrane, it is possible that such potentials also work in the case of the immunological synapses. It should be noted that, in the case of the higher elements of the immune system, the Th and Tc lymphocytes, the presentation is made only in the MHC cup to TCR / CD3 and it is not known why it cannot be done directly. The T lymphocytes have no antigen directly uptake receptors. There may be an electromagnetic potential at the level of these cups, which could have a role in the spatial presentation as well as in physical signaling , possibly also in the analysis of the antigen in terms of radiation or even in their cutting.
If the lymphocyte by TCR some how participates in the annihilation of the radioactive load of antigens, it would explain its continuous place in the top of the antineoplastic defence, along with NK, given that may not have activation from which seems defective in the recognition of the tumor antigens.
At the level of the central nervous system there are a multitude of neural formations with a cup-like structure and they may be related to the increased resistance of the cephalic extremity to X-rays, as radiologists do not need a protection helmet. This could be related to format of the callote cranienne , as well as the format of axile , the wrist and elbow , because the protection realize herself only with worn apron by radiologists and by radiotherapy patients or by pregnant women who need X-rays.
If, at the level of the nervous system, the transmission of the signals is made by action potentials and by electrical potential differences between the inside and outside of the cell, at the level of the immune system there is an interesting feature: the antigen processing takes place during “the trip” that APC makes from the entry place of infectious agents to the regional lymphoid organs (lymphatyc ganglions). The phenomenon is part of homing and it may be necessary to induce or involve potential differences in the normal making of immune responses, because it is not known why this move is necessarily needed.
Another argument of the physical impact on the immune system would be that stress is considered by many authors to be aggravating neoplasms by the immunosuppression of the immune system. The stress influences the nervous system by an electrical component, which may cause changes in the immune system.
It should be noted that at the level of the nervous system there is a double component in terms of the transmission of nerve influx: a physical one represented mainly by the propagation of action potentials at the level of neurons, whereas at the level of neuronal synapses there is interruption of physical contact between neurons. they do not touch and the mediation is done chemically through mediators. So there is a conversion of transmission from physical – chemical signals to chemical signals.
Similarly, in the case of the etiopathogenesis of neoplasms, there may be a conversion of a physical inducing signal that is not yet known to a chemical and physical progression signal that is described in oncology in “activation cascades.”
This signal may also be present in the neoplastic clone and the leukocytes, possibly extending or “jumping” from the first neoplastic cell to the first elements of the immune system that examined it, and then extended to all the leukocyte elements).
However, the signal from neoplastic cells is much more harmful and induces major organic and functional disorders of those cells. If it is present in the immune system, it is weaker or it is only a component of the inducing signal, which does not produce organic but only functional disorders (such as the electrical component of stress, which induces immunosuppression).
The T lymphocytes at the upper level (helper and regulatory) may not “see” the tumor antigens in the sense that they have established a pathological tolerance to them from the first neoplastic cell, a tolerance that extends to the entire malignant clone, including to the metastatic cells.
Parallelism between the immunological tolerance induced by pregnancy and tolerance in neoplasm
A type of tolerance that is not similar to this is also described only in pregnancy, where it is not known exactly the mechanism by which the egg cell immediately induces tolerance to the entire immune system, from the upper T lymphocytes to all the elements of the non-specific immune system because, immediately after the formation and nesting of the egg cell, it must be intact and not attacked by the local elements of the immune systems, especially the elements of the non-specific immune system that do not have the capacity to analyze as the elements of the specific immune system, given that pregnancy is a semiallograft or even an allograft in carrier mothers.
Subsequently tolerance extends to all the embryo-fetal cells until the delivery date, when it is lost at the age of 9 months, exceeding this age results in rejection, so it seems that it is a genetic program predetermined by species, given that for humans there is also an evolution variant of 7 months.
Tolerance is double: mother / foetus and foetus / mother and it last strictly only during pregnancy.
Classically, a multitude of hormonal, enzymatic, cytokine, protein and lipid molecules are described in the induction and keeping of pregnancy tolerance: progesterone, estrogen, chorionic gonadotrophin, proteases, collagenases, β-2 microglobulin, haptoglobin, uteroglobin, prostaglandin ,, cytokines with favorable action on the growth and development of the embryo-foetus: IL-1, IL-2, IL-3, IL-6, IL-8, TGFβ -2, interferon, GM-CSF.
One of the main cytokines with a repressive role is IL-10, produced by , by which it inhibits . The cytokine complex produced by the lymphocyte induces a regulation in the paracrine- type pregnancy.
IL-10 is the major cytokine and regulatory T lymphocyte , along with TGF-β, by which it controls excessive responses.
The tolerance to pregnancy starts immediately after the formation of the egg cell so that it is not destroyed. The rapidity with which it established suggests that the chemical system of the involved molecules may be doubled by a physical system, possibly signaling from the range of the electromagnetic signals.
The tolerance to pregnancy is a model of physiological tolerance and it would seem that the immune system “sees” the egg cell and all the embryo-fetal elements, it knows them well and that is why it gives them tolerance by an incompletely known mechanism. Tolerance is also double from the fetus for the mother until the age of 9 months.
Some authors argue in the induction of pregnancy tolerance the intervention of electronegative protection mechanisms, competitive absorption based on the saturation of the antigenic sites or the modification of antigenic expression by “the internalization of antigens”, offering as an example of electronegative protection the layer of mucopolysaccharides covering syncytiotrophoblast and that would show similarities to the one in some bacteria, in which mucopolysaccharides or capsular carbohydrates do not allow the antigenic recognition. All these hypotheses belong to the theory of masking the antigenic sites, which claim the impossibility to recognize the fetal HLA antigenes by the immune system. However, these theories are controversial because the antigenicity of the trophoblast has been demonstrated. The cells of the syncytiotrophoblast in normal pregnancy do not express the classical HLA molecules of class I or II. The cytotrophoblast cells at the villous level, immediately below the syncytiotrophoblast, do not express HLA of class I but they contain its corresponding mRNA. The extraviloseal cytotrophoblast at the level of the decidua, as well as the trophoblastic cells at the level of the chorion and the placental bed in the case of the term pregnancy express mRNA and HLA-G molecules (HLA class Ib antigen, nonpolymorphic), but also HLA-C and E. So, however, pregnancy is a semiallograft, which means that the mechanism of induction and maintenance of tolerance to pregnancy is extremely complex and intelligent, especially because it is double (it is also fetus –mother), it is natural, physiological and probably genetically predetermined for a period of 9 months.
In neoplasms, it seems that an inverse phenomenon of pathological tolerance occurs, by which the lymphocyte does not “see” and does not recognize neoplastic cells, and there is a defect in the uptake, processing and presentation of tumor antigens in the MHC-cup II of APC.
The blockage in seems to be only functional because the immune system, in most cases at least at the onset of the neoplasms, does not have immunodepression in most cases, whereas the other lines work normally (anti-infective, autoimmune).
There may be a signal on the lymphocyte that blocks its access to neoplastic antigens (so it does not “see” the malignant cells), but this it seems to have a weaker component than the inductive signal (S1) which is present on the malignant cells and causes so many organic disorders as well as functional ones. This signal from the elements of the immune system (which would be S2) and which produces only functional disorders, is much weaker than S1 (or it is only its component that passed on the leukocytes during the analysis they performed on the malignant cells).
If the inductive signal S1 is physical, then it may undergo a conversion (or an inversion) on a chemical type (“a signaling cascade” classically described in oncology), just as the signalling of potential action type at the level of the neurons is converted to signalling of chemical mediators at the level of the synaptic slits, where there is no physical contact.
Under these conditions, the two signals S1 from the malignant clone and S2 from the lymphocyte clone may have the same polarity (plus with plus or minus with minus), which would be a variant that could explain the incompatibility between them, so that the lymphocytes cannot recognize the neoplastic cells.
These theories would explain the duality of cancer, namely that the damage is both on the neoplastic clone and also on the immune system, on the lymphocyte clone that had the first contact with the first affected neoplastic cell.
From the clinical and paraclinical observations, these signals (S1 and S2 ) seem to have several main characteristics:
– in case all the neoplastic cells are eradicated (in situ extirpated neoplasms or “sterilizations” referred to in oncology in the case of leukemias or lymphomas treated chemically and by radiotherapy), it would seem that the inductive signal “leaps” (passes) to other cells belonging to the same tissue or even another tissue, so that recurrence still occurs after some years.
– in the case of dead neoplastic cells, possibly as the signal don’t by present on them , because vaccine immunotherapy trials have been performed on the killed neoplastic cells (ex. by Rx ) , but did not have satisfactory results. Interestingly, the nonspecific stimulation with microbial vaccines (eg. BCG antituberculosis vaccine) has improved in some forms of cancer better than neoplastic cell stimulation. This is an additional argument that the lymphocyte responds normally to other stimuli but does not “see” the neoplastic cells and cannot initiate a correct response.
One of the basic links may be antigens capture, the processing and the presentation of tumor antigens in APC, which has a mechanism that is still incompletely elucidated.
If the living tumor cells are indeed covered by a signal or have a particular mechanism by which they cannot be recognized by the immune system, the tumor antigens processed and presented by APC may come mostly from the dead neoplastic cells that probably lost their signal and can also be used as vaccines. If these tumor antigens coming from dead cells are mostly involved in the stimulation of the lymphocyte by APC, it would explain why its immune response is weak, as for detritus and it is not the expected one, ie. a strong immunological response to rejection of some completely aberrant, monstrous cells.
The IFN-γ, the main effector cytokine of the lymphocyte, is not very effective, so it does not seem to give an immunological response as for highly modified cells with great antigenicity, but rather a response as for some detritus (dead neoplastic cells ?).
After a variable period of the evolution of the neoplastic disease, the immunodepression starts, so probably the and lymphocyte (through the effector and help function ) does not consider adequate the major intervention of the other elements of the immune system because they do not “see” the tumor antigens. It is known that the number and the activity of the NK lymphocytes decreases in time, probably under the coordination of which it works as a suppressor .
Also, this could also explain the expected lack of response to some immunomodulatory therapies, such as fungal extracts or some monoclonal antibodies that could be blocked at the upper level by and which find unjustified the intervention of such powerful mechanisms in conditions in which they do not have adequate antigenic stimulation.
Th1 should intervene by non-exercityng correct of the fonction effector and help .
This would mean that the main defect is double, at the level of and .Treg has Th1 support (Treg is stimulated of Th1 by IL-2 ) .
In the absence of correct activation of the Th1 , the lymphocytes Tc can be deleted , so there is a major defect in the cellular defence at the higher level, which would explain the aggressiveness of the neoplastic disease and finally the invasion of the body by metastasis.
- Abbas A . K., Lichtman A. H. , Pillai S. , Basic Immunology : Functions and disorders of the immune system , Sixth edition , Elsevier 2020;
- Alunno A. , Carubbi F., Bistoni O., Caterbi S., Bartoloni E. , Mirabelli G., Cannarile F., Cipriani P., Giacomelli R., Gerli R. , Tregulatory and Thelper 17 Cells in Primary Sjogren’s Syndrome:Facts and Perspectives ,Volume 2015/ Article ID 243723/ htpps://doi.org/10.1155/2015/243723;
- Anghel R. ,Oncolgie generala , Editura Universitara ’’ Carol Davila ’’ , Bucuresti 2019;
- Badea R . I., Dudea S. M. , Mircea P.A. , Stamatian F., Tratat de ultrasonografie clinica , vol. 1 ,Editura Medicala Bucuresti ,2007
- Bara C. ,Activarea limfocitelor T -rolul moleculelor adaptator ,https://www.emcb.ro/article.php?story=20030614203140000;
- Bara C. , Esential de imunologie , Editura ALL , Bucuresti 2002;
- Blidaru I.E., Elemente de imunologie gestationala ,Institutul European ,2007;
- Carasevici E. , Dumitriu I. ,Cianga C. ,Cianga P., Zugun-Eloae F. , Imunologie , Universitatea de Medicina și Farmacie Gr.T .Popa Iasi 1999 ;
- Cianga P., Tehnici utilizate in imunologie- notiuni introductive ,Editura Pim , Iasi 2008;
- Covic M. , Stefanescu D. , Sandovici I. , Gorduza E.V. , Genetica Medicala , editia a III-a , Editura Polirom , Iasi 2017
- Cristea V., Imunologie Fundamentala, Editura Medicala Universitara “Iuliu Hatieganu “ Cluj Napoca 1999;
- Cristea V., Costin N., Crisan M., Olinescu A.: Imunologie clinică , Ed. Casa Cărții de știință ,Cluj-Napoca, 1999;
- Delves P.J. , Martin S.J. , Burton D.R., Roitt I.M. , Roitt’s Essential Immunology , Thirteenth edition , Wiley Blackwell , 2017;
- Dejica D.: Tratat de imunologie clinică , Ed. Dacia ,Cluj-Napoca ,1997;
- Fares J. , Fares M. , Khachfe H.H. ,Salhab H.A. , Fares Y. , Molecular principles of metastatic: a hallmark of cancer revisited , PMC7067809 DOI:10,1038/s41392-020-0134-x , PMC free-Pub Med;
- Fouad Y. A. , Aanei C . , Revisiting the hallmark of cancer , Am J Cancer Res. 2017; 7(5): 1016–1036 ;
- Gavrilita L ., Morfopatologie generala si speciala , Litografia UMF Iasi ,1991
- Hugher E., Scurr M., Campbell E.,James E., Godkin A., Gollimore . T-cell modulation by Cyclophosplamide for tumord therapy. Immunology. 2018 May ;154(1) :62-68. PMC free-Pub Med.;
- Iancu R. I. , Zara A. D. ,Mirestean C. C., Iancu D.P.T. , Radiomics in Head and Neck Cancers Radiotherapy .Promiser and Challanger . Maedica a Journal of Clinical Medicine No .3/ 2021 , 2021; 16(3): 482-488
- Kasper D.L., Fauci A.S. : Harrison’s infectious diseases, Second Edition , Editura All , 2020, Bucuresti;
- Kumar V., Abbas A. K. , Aster J. C., Robbins Basic Parthology, 9th Edition , Editura Medicala Callisto 2015;
- Manolescu N., Bolte S., Oncologie veterinara , Editura Ceres , Bucuresti ,1991
- Marineci C.D. , Chirita C. , Old and new in cancer treatment , Oncolog-Hematolog ro , Journal for continuing Medical Education , Editorial Group Medichub Media , 30 aprilie 2018 , DOI:10.26416/FARM.181.2.2018.1680;
- McHugh R. S. , Shevach E. M. ,The role of suppressor T cells in regulation of immune responses , Allergy Clin Immunol , 2002 Nov;110(5):693-702. PMID: 12417876 ,Doi : 10. 1067/mai.2002.129339
- Mihaescu G. , Chifiriuc C ., Imunologie si Imunopatologie , Editura Medicala , Bucuresti 2021;
- Miron L., Terapia oncologica: optiuni bazate pe dovezi , Institutul European ,Iasi 2008;
- Negru D. , Bostaca T. , Fotea V. , Jari I. , Ursaru M. , Ursulescu C. , Moisii L., Reut R., Radiologie si Imagistica Medicala ,Editura ’’ Gr.T. Popa ’’ ,UMF Iasi , 20
- Peretianu D. , Saragea M. M. : Imunologia in teoria si practca medicinei , vol II ,Editura All , Bucuresti 1998 ;
- Scurr M , Pembroke T , Bloom A , Roberts D , Thomas A , Smart K, , Bridge-man H. . Adams R , Brewster A , Jones R Gwynne ,S ,Blount ,Harrop R.,Hills, Gallimon, Godkin. A. : Low- Dose Cyclophosphamide Induces Anti-tumoral T Cell Responses ,which Associate with Survival în Metastatic Colo-rectal Cancer ; Clin . Cancer Res , 2017 Nov 15 23 (220 ;67716780 doi : 10 1158 / 1078-0432 PMCfree- PubMed;
- Voiculescu C., Pătrășcanu A., Voiculescu M., Hongeag M., Avramescu C., Vâlcea V., Radu E.: Noțiuni de imunologie și imunopatologie , Editura Academiei Române ,1999;
- YamaguchiT. , Sakaguchi S. , Regulatory Tcells in immune surveillance and treatment of cancer , Semin Cancer Biol . 2006 Apr; 16(2):115-23.doi:10.1016/j.semcancer.2005.11.005 . Epub 2006 Jan 11 . PMID : 16376102
- Zugun F.E . , Ivanov I. C. , Tehnici amplificative ( PCR ) si nonamplificative ( hibridizare in situ ) de analiza a acizilor nucleici in diagnosticul molecular .Editura Gr. T. Popa , Iasi 2013;